жң¬её–жңҖеҗҺз”ұ costa_na дәҺ 2013-12-5 15:57 зј–иҫ‘
+ ]- f7 Y" u) d. k3 n% [4 x8 y+ o9 y- u
1.2.иҒ”еҗҲеҢ–з–—ж–№жЎҲ" i) y/ e. p. ^; I* U$ t5 {* o0 I
5 d9 q; @0 R( F# h k
1.2.1.еҸҢиҚҜиҒ”еҗҲ4 n- X. p! y0 l- R! `4 m" y7 O3 L; b
6 W/ u. m& G2 K. f. ?7 F4 U" M
1. The Cochrane Collaboration group reviewed data from all randomized controlled trials published between January 1980 and June 2006, comparing a doublet regimen with a single-agent regimen or comparing a triplet regimen with a doublet regimen in patients with advanced NSCLC.[6] Sixty-five trials (13,601 patients) were identified., ]# ~( j' t, u
科е…ӢдјҰеҚҸдҪңз»„(Cochrane Collaboration group)еӣһйЎҫдәҶд»Һ1980е№ҙ1жңҲеҲ°2006е№ҙ6жңҲй—ҙе…¬еёғзҡ„жүҖжңүзҡ„еҜ№жҜ”з ”з©¶еҸҢиҚҜиҒ”еҗҲж–№жЎҲе’ҢеҚ•иҚҜж–№жЎҲжҲ–иҖ…дёүиҚҜиҒ”еҗҲж–№жЎҲе’ҢеҸҢиҚҜиҒ”еҗҲж–№жЎҲзҡ„еңЁжҷҡжңҹNSCLCжӮЈиҖ…дёӯеұ•ејҖзҡ„йҡҸжңәжҺ§еҲ¶дёҙеәҠиҜ•йӘҢгҖӮдёҖе…ұжңү65дёӘдёҙеәҠиў«зЎ®е®ҡгҖӮ
( W0 X" L' g: F& F. C0 _' u* y/ e& G$ N2 B' W/ Q1 m( V
a. In the trials comparing a doublet regimen with a single-agent regimen, a significant increase was observed in tumor response (odds ratio [OR], 0.42; 95% confidence interval [CI], 0.37вҖ“ 0.47; P < .001) and 1-year survival (OR, 0.80; 95% CI, 0.70вҖ“0.91; P < .001) in favor of the doublet regimen. The absolute benefit in 1-year survival was 5%, which corresponds to an increase in 1-year survival from 30% with a single-agent regimen to 35% with a doublet regimen. The rates of grades 3 and 4 toxic effects caused by doublet regimens were statistically increased compared with rates following single-agent therapy, with ORs ranging from 1.2 to 6.2. There was no increase in infection rates in doublet regimens.( ]2 L2 B4 z, c, _( C7 A
еңЁеҜ№жҜ”еҸҢиҚҜиҒ”еҗҲж–№жЎҲе’ҢеҚ•иҚҜж–№жЎҲзҡ„дёҙеәҠдёӯпјҢеңЁеҸҢиҚҜж–№жЎҲдёӯи§ӮеҜҹеҲ°дәҶиӮҝзҳӨе“Қеә”пјҲдјҳеҠҝжҜ”[OR], 0.42; 95%зҪ®дҝЎеҢәй—ҙ[CI], 0.37вҖ“0.47; P < .001пјүе’Ң1е№ҙз”ҹеӯҳзҺҮзҡ„жҳҫи‘—жҸҗй«ҳгҖӮз»қеҜ№зҡ„1е№ҙз”ҹеӯҳзҺҮиҺ·зӣҠжҳҜ5%пјҢе°ҶеҚ•иҚҜж–№жЎҲзҡ„1е№ҙз”ҹеӯҳзҺҮд»Һ30%жҸҗй«ҳеҲ°дәҶ35%гҖӮзӣёжҜ”еҚ•иҚҜж–№жЎҲпјҢз”ұеҸҢиҚҜж–№жЎҲеј•иө·зҡ„3-4зә§жҜ’еүҜдҪңз”Ёжңүз»ҹи®ЎеӯҰдёҠзҡ„еўһеҠ (OR, 1.2-6.2)гҖӮеҸҢиҚҜиҒ”еҗҲжІЎжңүеўһеҠ ж„ҹжҹ“зҺҮгҖӮ/ p7 l+ r" ^- x% g: p) h& W& e
# _. ?9 o2 e( B
b. There was no increase in 1-year survival (OR, 1.01; 95% CI, 0.85вҖ“1.21; P = .88) for triplet regimens versus doublet regimens. The median survival ratio was 1.00 (95% CI, 0.94вҖ“1.06; P = .97).* I% q4 s0 v" u0 @8 S* _6 M. ^
еңЁдёүиҚҜж–№жЎҲе’ҢеҸҢиҚҜж–№жЎҲзҡ„жҜ”иҫғдёӯпјҢ1е№ҙз”ҹеӯҳзҺҮжІЎжңүеҫ—еҲ°жҸҗй«ҳ(OR, 1.01; 95% CI, 0.85вҖ“1.21; P = .88)пјҢдёӯдҪҚз”ҹеӯҳзҺҮдёә1.00(95% CI, 0.94вҖ“1.06; P = .97)гҖӮ3 C2 s! E1 d0 ?
( e. P' o# }3 R! i) q6 a
1.2.2. йЎәй“ӮеҜ№жҜ”еҚЎй“Ӯ0 W6 c6 a8 F3 H3 u" p5 w, E
6 c) v/ e& t5 ?6 ^4 K
2. Several meta-analyses have evaluated whether cisplatin or carboplatin regimens are superior with variable results.[7,8,9] One meta-analysis reported individual patient data for 2,968 patients entered in nine randomized trials.[7]
7 A0 V5 ]8 D) _5 Y9 E. ?: Rе°‘ж•°иҚҹиҗғеҲҶжһҗиҜ„дј°дәҶжҳҜеҗҰйЎәй“ӮзӣёжҜ”еҚЎй“ӮжӣҙдјҳгҖӮдёҖдёӘиҚҹиҗғеҲҶжһҗжҠҘе‘ҠдәҶе…Ҙз»„9дёӘйҡҸжңәдёҙеәҠзҡ„2968еҗҚжӮЈиҖ…зҡ„еҚ•зӢ¬зҡ„дёӘдҪ“ж•°жҚ®пјҡ
! I. B, o7 ~& Y7 N! s7 a
0 Y" C) K2 n- }( h4 ?' X% M# Ha. The objective response rate was higher for patients treated with cisplatin than for patients treated with carboplatin (30% vs. 24%, respectively; OR, 1.37; 95% CI, 1.16вҖ“1.61; P < .001).% q; E D ?2 ^2 x
дҪҝз”ЁйЎәй“ӮжІ»з–—зҡ„жӮЈиҖ…дёӯпјҢе…¶е®ўи§Ӯе“Қеә”зҺҮй«ҳдәҺжҺҘеҸ—еҚЎй“Ӯзҡ„жӮЈиҖ…(30% vs. 24%, respectively; OR, 1.37; 95% CI, 1.16вҖ“1.61; P < .001)гҖӮ
- G- c0 W$ b$ Z+ Y/ B! j- r" C/ [3 C3 y5 \+ C
b. Carboplatin treatment was associated with a nonвҖ“statistically significant increase in the hazard of mortality relative to treatment with cisplatin (hazard ratio [HR], 1.07; 95% CI, 0.99вҖ“1.15; P = .100).: i9 o6 R" x4 ~4 Y r( `. u, u
зӣёеҜ№дәҺйЎәй“ӮпјҢеҚЎй“ӮжІ»з–—ж–№жЎҲдёҺйқһз»ҹи®ЎеӯҰеўһеҠ зҡ„жӯ»дәЎйЈҺйҷ©зӣёе…іпјҲйЈҺйҷ©жҜ” [HR], 1.07; 95% CI, 0.99вҖ“1.15; P = .100пјүгҖӮ, k7 H) I/ B& I) G
- Y& u7 G# M' {2 d* s* m# { F6 ~c. In patients with nonsquamous tumors and those treated with third-generation chemotherapy, carboplatin-based chemotherapy was associated with a statistically significant increase in mortality (HR, 1.12; 95% CI, 1.01вҖ“1.23 and HR, 1.11; 95% CI, 1.01вҖ“1.21, respectively).
7 j; r2 L1 M3 g9 g' OеңЁйқһйіһзҷҢ并且жҺҘеҸ—第дёүд»ЈеҢ–з–—иҚҜзү©жІ»з–—зҡ„жӮЈиҖ…дёӯпјҢеҹәдәҺеҚЎй“Ӯзҡ„еҢ–з–—дёҺз»ҹи®ЎеӯҰж„Ҹд№үдёҠжҳҫи‘—еўһеҠ зҡ„жӯ»дәЎзҺҮзӣёе…іпјҲHR, 1.12; 95% CI, 1.01вҖ“1.23 and HR, 1.11; 95% CI, 1.01вҖ“1.21, respectivelyпјүгҖӮ
6 x# j+ y4 r) L. V" v$ s V6 z7 j: h& w% T
d. Treatment-related toxic effects were also assessed in the meta-analysis. More thrombocytopenia was seen with carboplatin than with cisplatin (12% vs. 6%; OR, 2.27; 95% CI, 1.71вҖ“3.01; P < .001), while cisplatin caused more nausea and vomiting (8% vs. 18%; OR, 0.42; 95% CI, 0.33вҖ“0.53; P < .001) and renal toxic effects (0.5% vs. 1.5%; OR, 0.37; 95% CI, 0.15вҖ“0.88; P = .018).
/ c3 X) @, Q6 |/ Y& r' QжІ»з–—зӣёе…іжҜ’жҖ§еҗҢж ·еңЁиҚҹиҗғеҲҶжһҗдёӯеҫ—еҲ°иҜ„дј°гҖӮзӣёжҜ”йЎәй“ӮпјҢеҚЎй“ӮжӣҙеӨҡзҡ„еҮәзҺ°иЎҖе°ҸжқҝеҮҸе°‘пјҲ12% vs. 6%; OR, 2.27; 95% CI, 1.71вҖ“3.01; P < .001пјүпјҢдҪҶйЎәй“ӮеҜјиҮҙжӣҙеӨҡзҡ„жҒ¶еҝғе’Ңе‘•еҗҗпјҲ8% vs. 18%; OR, 0.42; 95% CI, 0.33вҖ“0.53; P < .00пјүпјҢд»ҘеҸҠиӮҫи„ҸжҜ’жҖ§пјҲ0.5% vs. 1.5%; OR, 0.37; 95% CI, 0.15вҖ“0.88; P = .018пјүгҖӮ/ ~$ t F, Z! _! f3 y9 e
) z% P6 p( o* P) D; C6 r O
e. The authors concluded that treatment with cisplatin was not associated with a substantial increase in the overall risk of severe toxic effects. This comprehensive individual-patient meta-analysis is consistent with the conclusions of other meta-analyses, which were based on essentially the same clinical trials but which used only published data.
" w- t( R! G X7 lдҪңиҖ…жҖ»з»“еҲ°йҮҮз”ЁйЎәй“Ӯзҡ„иҒ”еҗҲ治疗并жңӘжңүдёҘйҮҚжҜ’еүҜдҪңз”Ёзҡ„жҳҫи‘—еўһеҠ гҖӮиҝҷдёӘе№ҝжіӣзҡ„еҚ•дёӘжӮЈиҖ…зҡ„иҚҹиҗғеҲҶжһҗдёҺе…¶д»–еҹәдәҺеҗҢж ·зҡ„дёҙеәҠдҪҶеҸӘйҮҮзәіе…¬еёғзҡ„ж•°жҚ®зҡ„иҚҹиҗғеҲҶжһҗз»“и®әдёҖиҮҙгҖӮ9 _# _. [" H" G* O4 U; j( O) O
1 f( R: |% l& g$ `9 ]5 [
1.2.3. й“Ӯзұ»еҜ№жҜ”йқһй“Ӯзұ»
0 L" p; T4 V) h% k O1 Q2 L; z7 ~8 w8 ^2 l2 ^! y
3. Three literature-based meta-analyses have trials comparing platinum with nonplatinum combinations.[10,11,12]
; f" p) W' X. @# q: N F0 vдёүдёӘеҹәдәҺж–ҮзҢ®зҡ„иҚҹиҗғеҲҶжһҗеҜ№жҜ”дәҶй“Ӯзұ»е’Ңйқһй“Ӯзұ»зҡ„иҒ”еҗҲж–№жЎҲпјҡ
: X3 M5 x. M- U6 q
& ~' w S' R8 {; }, G. f" ta. The first meta-analysis identified 37 assessable trials that included 7,633 patients.[10]
$ ~& p0 g$ T+ S/ @7 B* s5 k第дёҖдёӘиҚҹиҗғеҲҶжһҗз ”з©¶дәҶ37дёӘеҢ…еҗ«7633дҪҚжӮЈиҖ…зҡ„еҸҜиҜ„дј°дёҙеәҠ8 T1 c" R, J, W
• A 62% increase in the OR for response was attributable to platinum-based therapy (OR, 1.62; 95% CI, 1.46вҖ“1.8; P < .001). The 1-year survival rate was increased by 5% with platinum-based regimens (34% vs. 29%; OR, 1.21; 95% CI, 1.09вҖ“1.35; P = .003).
7 w/ A2 H. F0 c& M9 s" vеңЁй“Ӯзұ»иҒ”еҗҲжІ»з–—дёӯпјҢз–ҫз—…е“Қеә”зҺҮзҡ„дјҳеҠҝжҜ”жңү62%зҡ„жҸҗй«ҳпјҲOR, 1.62; 95% CI, 1.46вҖ“1.8; P < .001пјүпјҢ1е№ҙз”ҹеӯҳзҺҮжңү5%зҡ„еўһеҠ пјҲ34% vs. 29%; OR, 1.21; 95% CI, 1.09вҖ“1.35; P = .003пјүгҖӮ# K* M1 I$ c U- P1 M% }3 ]
% M6 b& O, Q5 o: A9 \- N1 A" B• No statistically significant increase in 1-year survival was found when platinum therapies were compared with third-generation-based combination regimens (OR, 1.11; 95% CI, 0.96вҖ“1.28; P = .17).
" L& F1 L3 Y! E7 \# Q0 ZеҜ№жҜ”й“Ӯзұ»е’Ң第дёүд»ЈиҒ”еҗҲз”ЁиҚҜж–№жЎҲпјҢ1е№ҙз”ҹеӯҳзҺҮжІЎжңүз»ҹи®ЎеӯҰж„Ҹд№үдёҠзҡ„жҳҫи‘—еўһеҠ пјҲOR, 1.11; 95% CI, 0.96вҖ“1.28; P = .17пјүгҖӮ: [; I7 K5 x6 A& I' A1 t7 {
# z8 e% [! V( g4 g' h• The toxic effects of platinum-based regimens was significantly higher for hematologic toxic effects, nephrotoxic effects, and nausea and vomiting but not for neurologic toxic effects, febrile neutropenia rate, or toxic death rate. These results are consistent with the second literature-based meta-analysis.
& }. I6 z) r& n6 aеҹәдәҺй“Ӯзұ»зҡ„иҒ”еҗҲж–№жЎҲпјҢеңЁиЎҖж¶ІеӯҰжҜ’жҖ§гҖҒиӮҫжҜ’жҖ§е’ҢжҒ¶еҝғе‘•еҗҗзӯүеүҜдҪңз”Ёж–№йқўйғҪжңүжҳҫи‘—зҡ„еўһеҠ пјҢдҪҶзҘһз»ҸжҜ’жҖ§гҖҒеҸ‘зғӯжҖ§дёӯжҖ§зІ’з»ҶиғһеҮҸе°‘е’ҢжҜ’жҖ§зӣёе…іжӯ»дәЎзҺҮж–№йқўжІЎжңүеўһеҠ гҖӮиҝҷдәӣз»“жһңдёҺ第дәҢдёӘеҹәдәҺж–ҮзҢ®зҡ„иҚҹиҗғеҲҶжһҗдёҖиҮҙгҖӮ% l4 }. {- N: s% u/ o
! e8 [" f9 @4 t4 h) r9 ~b. The second meta-analysis identified 17 trials that included 4,920 patients.[11]6 W; m! l+ ?& [% Z& H& E
第дәҢдёӘиҚҹиҗғеҲҶжһҗз ”з©¶дәҶ17дёӘеҢ…еҗ«4920дҪҚжӮЈиҖ…зҡ„дёҙеәҠ
7 c2 ^ R E1 j- R4 f! v• The use of platinum-based doublet regimens was associated with a slightly higher survival at 1 year (relative risk [RR], 1.08; 95% CI, 1.01%вҖ“1.16%; P = .03) and a better partial response (RR, 1.11; 95% CI, 1.02вҖ“1.21; P = .02), with a higher risk of anemia, nausea, and neurologic toxic effects
; }, `! Q9 l7 Y& G3 WдҪҝз”Ёй“Ӯзұ»зҡ„еҸҢиҚҜж–№жЎҲпјҢ1е№ҙз”ҹеӯҳзҺҮе…·жңүиҪ»еҫ®зҡ„жҸҗй«ҳпјҲзӣёеҜ№йЈҺйҷ©[RR], 1.08; 95% CI, 1.01%вҖ“1.16%; P = .03пјүпјҢдё”е…·жңүжӣҙдҪізҡ„йғЁеҲҶзј“и§ЈзҺҮпјҲRR, 1.11; 95% CI, 1.02вҖ“1.21; P = .02пјүпјҢдҪҶеҗҢж—¶дјҙйҡҸжӣҙй«ҳйЈҺйҷ©зҡ„иҙ«иЎҖгҖҒе‘•еҗҗе’ҢзҘһз»ҸеӯҰжҜ’жҖ§гҖӮ# R: ]" b7 [0 F: m" e
6 u6 `9 R" O) b& Y, y/ a
• In subanalyses, cisplatin-based doublet regimens improved survival at 1 year (RR, 1.16%; 95% CI, 1.06вҖ“1.27; P = .001), complete response (RR, 2.29; 95% CI, 1.08вҖ“4.88; P = .03), and partial response (RR, 1.19; 95% CI, 1.07вҖ“1.32; P = .002), with an increased risk of anemia, neutropenia, neurologic toxic effects, and nausea2 _3 i' I/ B. o% _7 x6 z# T, ]
еңЁдәҡз»„еҲҶжһҗдёӯпјҢеҹәдәҺйЎәй“Ӯзҡ„еҸҢиҚҜиҒ”еҗҲж–№жЎҲжҸҗй«ҳдәҶ1е№ҙз”ҹеӯҳзҺҮпјҲRR, 1.16%; 95% CI, 1.06вҖ“1.27; P = .001пјүгҖҒе®Ңе…Ёзј“и§ЈзҺҮпјҲRR, 2.29; 95% CI, 1.08вҖ“4.88; P = .03пјүгҖҒд»ҘеҸҠйғЁеҲҶзј“и§ЈзҺҮпјҲRR, 1.19; 95% CI, 1.07вҖ“1.32; P = .002пјүпјҢдҪҶеўһеҠ дәҶиҙ«иЎҖгҖҒдёӯжҖ§зІ’з»ҶиғһеҮҸе°‘гҖҒзҘһз»ҸжҖ§жҜ’жҖ§е’Ңе‘•еҗҗзҡ„йЈҺйҷ©гҖӮ) \$ U$ ?9 C1 L+ `% G3 F) u. _
) M3 o' a' ?7 ?# @/ ?• Conversely, carboplatin-based doublet regimens did not increase survival at 1 year (RR, 0.95; 95% CI, 0.85вҖ“1.07; P = .43)5 ?- c8 b6 P: v- L
зӣёеҸҚзҡ„жҳҜпјҢиҒ”еҗҲеҚЎй“Ӯзҡ„еҸҢиҚҜж–№жЎҲ并жңӘеўһеҠ 1е№ҙз”ҹеӯҳзҺҮпјҲRR, 0.95; 95% CI, 0.85вҖ“1.07; P = .43пјүгҖӮ% V- y B8 v+ Y4 j' W
/ r; ~$ o# M+ x1 F. p& Qc. The third meta-analysis of phase III trials randomizing platinum-based versus nonplatinum combinations as first-line chemotherapy identified 14 trials.[12] Experimental arms were gemcitabine and vinorelbine (n = 4), gemcitabine and taxane (n = 7), gemcitabine and epirubicin (n = 1), paclitaxel and vinorelbine (n = 1), and gemcitabine and ifosfamide (n = 1). This meta-analysis was limited to the set of 11 phase III studies that used a platinum-based doublet (2,298 and 2,304 patients in platinum-based and nonplatinum arms, respectively).' k7 z5 |4 F8 s7 U ~; ?0 p7 f
第дёүдёӘиҚҹиҗғеҲҶжһҗеҹәдәҺ14дёӘIIIжңҹзҡ„йҡҸжңәеҜ№жҜ”й“Ӯзұ»е’Ңйқһй“Ӯзұ»дёҖзәҝжІ»з–—зҡ„дёҙеәҠгҖӮиҜ•йӘҢз»„еҢ…жӢ¬еҗүиҘҝд»–ж»Ёе’Ңй•ҝжҳҘз‘һж»ЁпјҲn=4пјүпјҢеҗүиҘҝд»–ж»Ёе’Ңзҙ«жқүзғ·пјҲn=7пјүпјҢеҗүиҘҝд»–ж»Ёе’ҢиЎЁжҹ”жҜ”жҳҹпјҲn=1пјүпјҢзҙ«жқүйҶҮе’Ңй•ҝжҳҘз‘һж»ЁпјҲn=1пјүд»ҘеҸҠеҗүиҘҝд»–ж»Ёе’ҢејӮзҺҜзЈ·й…°иғәпјҲn=1пјүгҖӮиҜҘиҚҹиҗғеҲҶжһҗиў«йҷҗеҲ¶дәҺ11дёӘдҪҝз”Ёй“Ӯзұ»зҡ„IIIжңҹз ”з©¶пјҲ2298дҪҚжӮЈиҖ…дҪҝз”Ёй“Ӯзұ»жІ»з–—пјҢ2304дҪҚжӮЈиҖ…дҪҝз”Ёйқһй“Ӯзұ»жІ»з–—пјүгҖӮ
& e; v- T& J+ s% n" P• Patients treated with a platinum-based regimen benefited from a statistically significant reduction in the risk of death at 1 year (OR, 0.88; 95% CI, 0.78вҖ“0.99; P = .044) and a lower risk of being refractory to chemotherapy (OR, 0.87; CI, 0.73вҖ“0.99; P = .049). ^( Y4 ^. O {3 r+ R3 `% j6 \
еҹәдәҺй“Ӯзұ»жІ»з–—зҡ„жӮЈиҖ…еҸ—зӣҠдәҺз»ҹи®ЎеӯҰж„Ҹд№үдёҠжҳҫи‘—йҷҚдҪҺзҡ„1е№ҙжӯ»дәЎйЈҺйҷ©пјҲOR, 0.88; 95% CI, 0.78вҖ“0.99; P = .044пјүпјҢд»ҘеҸҠе…·жңүжӣҙдҪҺзҡ„еҜ№еҢ–з–—еӨҚеҸ‘зҡ„йЈҺйҷ©пјҲOR, 0.87; CI, 0.73вҖ“0.99; P = .049пјүгҖӮ% A' J T" k9 e; e9 E0 `2 _+ v
: R) o7 y" _7 P& k9 Y+ a* o
• •Forty-four (1.9%) and 29 (1.3%) toxic-related deaths were reported for platinum-based and nonplatinum regimens, respectively (OR, 1.53; CI, 0.96вҖ“2.49; P = 0.08). An increased risk of grade 3-4 gastrointestinal and hematologic toxic effects for patients treated with platinum-based chemotherapy was statistically demonstrated. There was no statistically significant increase in risk of febrile neutropenia (OR, 1.23; CI, 0.94вҖ“1.60; P = .063)
: l7 w" R9 l) }7 U41дҪҚпјҲ11.9%пјүе’Ң29дҪҚпјҲ1.3пјүеҲҶеҲ«жҺҘеҸ—й“Ӯзұ»е’Ңйқһй“Ӯзұ»жІ»з–—зҡ„жӮЈиҖ…жӯ»дәҺжҜ’жҖ§зӣёе…ізҡ„жӯ»дәЎдәӢ件пјҲOR, 1.53; CI, 0.96вҖ“2.49; P = 0.08пјүгҖӮеҹәдәҺй“Ӯзұ»зҡ„жІ»з–—иЎЁзҺ°еҮәеҜ№дәҺжӮЈиҖ…зҡ„3-4зә§иғғиӮ йҒ“жҜ’жҖ§е’ҢиЎҖж¶ІеӯҰжҜ’жҖ§еўһеҠ зҡ„йЈҺйҷ©гҖӮдҪҶжңӘжҳҫи‘—еўһеҠ еҸ‘зғӯжҖ§дёӯжҖ§зІ’з»ҶиғһеҮҸе°‘зҡ„йЈҺйҷ©пјҲOR, 1.23; CI, 0.94вҖ“1.60; P = .063пјүгҖӮ
& M5 |8 b! a/ a) v4 C; |7 m2 s* d1 _& K* K$ ]$ U
1.2.4. еүӮйҮҸе’Ңз»ҷиҚҜж–№жЎҲ
( D% e+ ?" q3 ]% B! Y* t6 T' R* B( |1 p7 Z( N* K) Q4 G
Among the active combinations, definitive recommendations regarding drug dose and schedule cannot be made, with the exception of pemetrexed for patients with adenocarcinoma.
" g, w" w" w# K3 s1 M2 [ XеңЁжңүж•Ҳзҡ„иҒ”еҗҲж–№жЎҲдёӯпјҢиҚҜзү©еүӮйҮҸе’Ңз»ҷиҚҜж–№жЎҲжІЎжңүжңҖз»Ҳзҡ„жҺЁиҚҗж„Ҹи§ҒпјҢе…¶дёӯдёҖдёӘдҫӢеӨ–жҳҜе»әи®®е°Ҷеҹ№зҫҺжӣІиөӣеә”з”ЁдәҺиӮәи…әзҷҢжӮЈиҖ…дёӯгҖӮ
7 l+ d. h1 O; w) p2 _1 A$ ~2 `3 v% u9 b2 R! o) E2 O! A
Evidence (drug and dose schedule):
& v- }0 X3 e/ t% ^) RиҜҒжҚ®пјҲеүӮйҮҸе’Ңз»ҷиҚҜж–№жЎҲпјүпјҡ" a {0 [9 x3 f8 m4 Y' C! D
1. There has been one meta-analysis of seven trials that included 2,867 patients to assess the benefit of docetaxel versus vinorelbine.[13] Docetaxel was administered with a platinum agent in three trials, with gemcitabine in two trials, or as monotherapy in two trials. Vinca alkaloid (vinorelbine in six trials and vindesine in one trial) was administered with cisplatin in six trials or alone in one trial./ Q# g/ t% u/ O
еҜ№7дёӘеҢ…жӢ¬2867еҗҚжӮЈиҖ…зҡ„дёҙеәҠзҡ„иҚҹиҗғеҲҶжһҗиҜ„дј°дәҶеӨҡиҘҝд»–иөӣеҜ№жҜ”й•ҝжҳҘз‘һж»Ёзҡ„收зӣҠгҖӮеӨҡиҘҝд»–иөӣеңЁдёүдёӘдёҙеәҠдёӯиҒ”еҗҲй“Ӯзұ»пјҢеңЁдёӨдёӘдёҙеәҠдёӯиҒ”еҗҲеҗүиҘҝд»–ж»ЁпјҢеңЁеҸҰдёӨдёӘдёҙеәҠдёӯдҪңеҚ•иҚҜеә”з”ЁгҖӮй•ҝжҳҘиҠұзўұеңЁе…ӯдёӘдёҙеәҠдёӯиҒ”еҗҲйЎәй“ӮпјҢеңЁдёҖдёӘдёҙеәҠдёӯдҪңеҚ•иҚҜеә”з”ЁгҖӮ
+ e% j, p( {& k: Z# M9 V• The pooled estimate for overall survival (OS) showed an 11% improvement in favor of docetaxel (HR, 0.89; 95% CI, 0.82вҖ“0.96; P = .004). Sensitivity analyses that considered only vinorelbine as a comparator or only the doublet regimens showed similar improvements.: W! ~; z; U! {6 o
еӨҡиҘҝд»–иөӣиЎЁзҺ°еҮәдәҶеҜ№еҗҲ并估算зҡ„жҖ»з”ҹеӯҳжңҹжңү11%зҡ„жҸҗй«ҳпјҲHR, 0.89; 95% CI, 0.82вҖ“0.96; P = .004пјүгҖӮж•Ҹж„ҹжҖ§еҲҶжһҗжҳҫзӨәй•ҝжҳҘз‘һж»ЁдҪңиҒ”еҗҲз”ЁиҚҜе’ҢеҚ•иҚҜе…·жңүзӣёдјјзҡ„з”ҹеӯҳжңҹж”№е–„гҖӮ
+ A- r6 l7 Z2 \% Y' j- c: O; m, }+ R! K! Y+ C
• Grade 3 to 4 neutropenia and grade 3 to 4 serious adverse events were less frequent with docetaxel-based regimens versus vinca alkaloid-based regimens (OR, 0.59; 95% CI, 0.38вҖ“0.89; P = .013 and OR, 0.68; 95% CI, 0.55вҖ“0.84; P < .001, respectively).) {4 ?/ ?) f7 G
еҜ№жҜ”й•ҝжҳҘиҠұзўұиҒ”еҗҲж–№жЎҲпјҢеӨҡиҘҝд»–иөӣиҒ”еҗҲж–№жЎҲе…·жңүиҫғдҪҺйў‘зҺҮзҡ„3-4зә§дёӯжҖ§зІ’з»ҶиғһеҮҸе°‘е’Ң3-4зә§зҡ„дёҘйҮҚеүҜдҪңз”ЁдәӢ件еҸ‘з”ҹзҺҮпјҲOR, 0.59; 95% CI, 0.38вҖ“0.89; P = .013 and OR, 0.68; 95% CI, 0.55вҖ“0.84; P < .001, respectivelпјүгҖӮ
/ q ]4 \( m+ q$ S9 M6 q
' V: e) o W z2. There have been two randomized trials comparing weekly versus every 3 weeks' dosing of paclitaxel and carboplatin, which reported no significant difference in efficacy and better tolerability for weekly administration.[14,15] Although meta-analyses of randomized controlled trials suggest that cisplatin combinations may be superior to carboplatin or nonplatinum combinations, the clinical relevance of the differences in efficacy must be balanced against the anticipated tolerability, logistics of administration, and familiarity of the medical staff for treatment decisions for individual patients. L. z2 a# ^0 b' v; c( f' R
е·Із»ҸжңүдёӨдёӘеҜ№жҜ”зҙ«жқүйҶҮиҒ”еҗҲеҚЎй“ӮжҜҸе‘Ёз»ҷиҚҜе’ҢжҜҸдёүе‘Ёз»ҷиҚҜзҡ„йҡҸжңәдёҙеәҠиҜ•йӘҢпјҢжҠҘе‘ҠжҳҫзӨәзӣёеҜ№йҖҡеёёзҡ„жҜҸдёүе‘Ёз»ҷиҚҜж–№жЎҲпјҢжҜҸе‘Ёз»ҷиҚҜеңЁжңүж•ҲжҖ§е’ҢжӣҙеҘҪзҡ„иҖҗеҸ—жҖ§ж–№йқўжІЎжңүжҳҫи‘—зҡ„е·®еҲ«гҖӮиҷҪ然еҜ№дәҺйҡҸжңәжҺ§еҲ¶дёҙеәҠзҡ„иҚҹиҗғеҲҶжһҗе»әи®®йЎәй“ӮдјҳдәҺеҚЎй“ӮжҲ–йқһй“Ӯзұ»зҡ„иҒ”еҗҲпјҢдҪҶжңүж•ҲжҖ§е·®ејӮзҡ„дёҙеәҠзӣёе…іжҖ§еҝ…йЎ»и°ғж•ҙжңҹжңӣзҡ„иҖҗеҸ—жҖ§гҖҒзү©жөҒз®ЎзҗҶгҖҒеңЁйҖүжӢ©жӮЈиҖ…ж—¶еҜ№еҢ»жҠӨдәәе‘ҳзҡ„зҶҹжӮүзЁӢеәҰзӯүеұһжҖ§гҖӮ) ^; E+ W& _- D, [
9 K7 L% p0 Y! g @ g8 Q
3. A large, noninferiority, phase III randomized study compared the OS in 1,725 chemotherapy-naive patients with stage IIIB or IV NSCLC and a PS of 0 to 1.[16] Patients received cisplatin 75 mg/m2 on day 1 and gemcitabine 1,250 mg/m2 on days 1 and 8 (n = 863) or cisplatin 75 mg/m2and pemetrexed 500 mg/m2 on day 1 (n = 862) every 3 weeks for up to six cycles.# ]( Y g+ f' X
дёҖдёӘеӨ§еһӢзҡ„йқһеҠЈж•ҲжҖ§phase IIIзҡ„йҡҸжңәз ”з©¶жҜ”иҫғдәҶеңЁIIIbжңҹжҲ–иҖ…IVжңҹжңӘз»ҸиҝҮеҢ–з–—дё”дҪ“иғҪиҜ„еҲҶдёә0-1еҲҶзҡ„NSCLCжӮЈиҖ…дёӯзҡ„жҖ»з”ҹеӯҳж—¶й—ҙгҖӮжӮЈиҖ…жҺҘеҸ—еңЁжҜҸ3е‘ЁдёәдёҖдёӘз–—зЁӢзҡ„е‘ЁжңҹеҶ…пјҢеңЁз¬¬1еӨ©жҺҘеҸ—йЎәй“Ӯ75mg/гҺЎиҒ”еҗҲ第1еӨ©е’Ң第8еӨ©жҺҘеҸ—еҗүиҘҝд»–ж»Ё1250mg/гҺЎпјҲn = 863пјүжҲ–иҖ…жҳҜеңЁз¬¬1еӨ©жҺҘеҸ—йЎәй“Ӯ75mg/гҺЎиҒ”еҗҲеҹ№зҫҺжӣІеЎһ500mg/гҺЎпјҲn = 862пјүпјҢжҢҒз»ӯжІ»з–—6дёӘз–—зЁӢгҖӮ7 ^! c7 r, A0 G: N2 X0 b3 W( K
• OS for cisplatin and pemetrexed was noninferior to cisplatin and gemcitabine (median survival, 10.3 mo vs. 10.3 mo, respectively; HR, 0.94; 95% CI, 0.84%вҖ“1.05%).5 d- [$ A* _ P/ X1 Y- T
жҺҘеҸ—йЎәй“ӮиҒ”еҗҲеҹ№зҫҺзҡ„жӮЈиҖ…пјҢе…¶OSдёҚеҠЈдәҺжҺҘеҸ—йЎәй“ӮиҒ”еҗҲеҗүиҘҝд»–ж»Ёзҡ„жӮЈиҖ…пјҲдёӯдҪҚз”ҹеӯҳжңҹпјҢ10.3дёӘжңҲ vs. 10.3дёӘжңҲпјӣHR, 0.94; 95% CI, 0.84%вҖ“1.05%пјү' q$ g. {2 z) W* W4 ?$ |: C8 P
0 ^( B3 ^$ E$ z# b+ J• OS was statistically superior for cisplatin and pemetrexed versus cisplatin and gemcitabine in patients with adenocarcinoma (n = 847; 12.6 mo vs. 10.9 mo, respectively) and large cell carcinoma histology (n = 153; 10.4 mo vs. 6.7 mo, respectively).6 Q1 Y6 X/ k `! G5 S- @
еңЁиӮәи…әзҷҢпјҲn = 847; 12.6дёӘжңҲ vs. 10.9дёӘжңҲ, respectivelyпјүе’ҢеӨ§з»ҶиғһзҷҢжӮЈиҖ…пјҲn = 153; 10.4дёӘжңҲvs. 6.7дёӘжңҲпјүдёӯпјҢйЎәй“ӮиҒ”еҗҲеҹ№зҫҺжӣІеЎһжҖ»жҳҜдјҳдәҺйЎәй“ӮиҒ”еҗҲеҗүиҘҝд»–ж»ЁгҖӮ
9 ^# L' [8 I$ r2 z! V$ V4 H/ I
) x; I! @+ ~3 h& L6 p" b) k$ Z• In contrast, in patients with squamous cell histology, there was a significant improvement in survival with cisplatin and gemcitabine versus cisplatin and pemetrexed (n = 473; 10.8 mo vs. 9.4 mo, respectively). For cisplatin and pemetrexed, rates of grade 3 or 4 neutropenia, anemia, and thrombocytopenia (P вүӨ .001); febrile neutropenia (P = .002); and alopecia (P < .001) were significantly lower, whereas grade 3 or 4 nausea (P = .004) was more common.
5 {# F3 d4 G' r& DзӣёеҜ№зҡ„пјҢеңЁиӮәйіһзҷҢжӮЈиҖ…дёӯпјҢйЎәй“ӮиҒ”еҗҲеҗүиҘҝд»–ж»ЁеҜ№жҜ”йЎәй“ӮиҒ”еҗҲеҹ№зҫҺжӣІеЎһпјҢжҖ»з”ҹеӯҳжңҹжңүжҳҫи‘—зҡ„жҸҗй«ҳпјҲn = 473; 10.8дёӘжңҲ vs. 9.дёӘжңҲпјүгҖӮеҜ№дәҺйЎәй“ӮиҒ”еҗҲеҹ№зҫҺжӣІеЎһж–№жЎҲжқҘиҜҙпјҢ3-4зә§зҡ„дёӯжҖ§зІ’з»ҶиғһеҮҸе°‘гҖҒиҙ«иЎҖгҖҒиЎҖе°ҸжқҝеҮҸе°‘пјҢд»ҘеҸҠеҸ‘зғӯжҖ§дёӯжҖ§зІ’з»ҶиғһеҮҸе°‘е’Ңи„ұеҸ‘йғҪжңүжҳҫи‘—зҡ„йҷҚдҪҺпјҢжңҖеёёи§Ғзҡ„еүҜдҪңз”Ёдёә3-4зә§зҡ„е‘•еҗҗгҖӮ
: m; r$ O; C7 g$ Q- h1 ]& @( [2 O6 o8 K$ m9 v
• This study suggests that cisplatin and pemetrexed are another alternative doublet for first-line chemotherapy for advanced NSCLC and also suggests that there may be differences in outcome depending on histology." A6 d& h9 z- I$ I, ]- g+ f
иҜҘз ”з©¶е»әи®®еҜ№дәҺжҷҡжңҹNSCLCжӮЈиҖ…жқҘиҜҙпјҢйЎәй“ӮиҒ”еҗҲеҹ№зҫҺжӣІеЎһжҳҜеҸҜйҖүзҡ„дёҖзәҝеҢ–з–—иҒ”еҗҲж–№жЎҲпјҢдҪҶж №жҚ®з»„з»ҮеӯҰе·®ејӮеҸҜиғҪжңүдёҚеҗҢзҡ„收зӣҠгҖӮ
$ Z' `' M7 W2 W5 f0 ?( k& k5 L5 y' ?" C+ d1 w: L1 C4 h( W, r6 ^7 s5 ?
*: зҝ»иҜ‘еҸҜиғҪжңүиҜҜ |
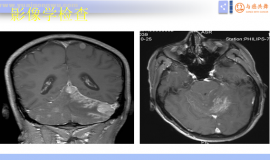

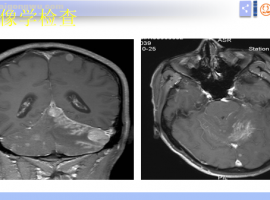 и„‘иҶңиҪ¬з§»иҜҠз–—жҪҳжҢҜе®Үж•ҷжҺҲ科жҷ®жҖ»з»“
и„‘иҶңиҪ¬з§»иҜҠз–—жҪҳжҢҜе®Үж•ҷжҺҲ科жҷ®жҖ»з»“
и„‘иҶңиҪ¬з§» дёӯдҪҚжІ»з–—з”ҹеӯҳжңҹ 3-6жңҲ
и„‘иҶңиҪ¬з§»зҡ„дёҙеәҠиЎЁзҺ°
и„‘иҶңиҪ¬з§»иҜҠз–—жҪҳжҢҜе®Үж•ҷжҺҲ科жҷ®жҖ»з»“
и„‘иҶңиҪ¬з§»иҜҠз–—жҪҳжҢҜе®Үж•ҷжҺҲ科жҷ®жҖ»з»“
и„‘иҶңиҪ¬з§» дёӯдҪҚжІ»з–—з”ҹеӯҳжңҹ 3-6жңҲ
и„‘иҶңиҪ¬з§»зҡ„дёҙеәҠиЎЁзҺ°
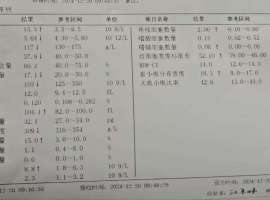 зҲ¶дәІдјҸзҫҺ+第еҚҒж¬ЎеҢ–з–—пјҲеҹ№зҫҺ +иҙқдјҗпјү
зҲ¶дәІжҜҸж¬ЎеҢ–з–—еҗҺзҡ„иЎҖ常规йғҪдёҚеӨ§еҘҪпјҢиҰҒеҺ»жү“зҷҪд»Ӣзҙ жҲ–иҖ…еҸЈжңҚжө·жӣІжіҠеё•еҚҮиЎҖе°ҸжқҝгҖӮдёҠж¬ЎеҢ–з–—е®Ң
зҲ¶дәІдјҸзҫҺ+第еҚҒж¬ЎеҢ–з–—пјҲеҹ№зҫҺ +иҙқдјҗпјү
зҲ¶дәІжҜҸж¬ЎеҢ–з–—еҗҺзҡ„иЎҖ常规йғҪдёҚеӨ§еҘҪпјҢиҰҒеҺ»жү“зҷҪд»Ӣзҙ жҲ–иҖ…еҸЈжңҚжө·жӣІжіҠеё•еҚҮиЎҖе°ҸжқҝгҖӮдёҠж¬ЎеҢ–з–—е®Ң
 дёӯиҚҜдјҡи®©йқ¶еҗ‘иҚҜз–—ж•ҲйҷҚдҪҺ90%пјҹ
дҪңиҖ…пјҡV
еүҚеҮ еӨ©пјҢжҲ‘еңЁжүӢжңәдёҠзңӢеҲ°дёҖзҜҮжҺЁж–ҮпјҢд№ҚдёҖзңӢж ҮйўҳвҖ”вҖ”гҖҠиӯҰжғ•пјҒпјҒдёӯиҚҜдјҡдҪҝйқ¶еҗ‘иҚҜзҡ„
дёӯиҚҜдјҡи®©йқ¶еҗ‘иҚҜз–—ж•ҲйҷҚдҪҺ90%пјҹ
дҪңиҖ…пјҡV
еүҚеҮ еӨ©пјҢжҲ‘еңЁжүӢжңәдёҠзңӢеҲ°дёҖзҜҮжҺЁж–ҮпјҢд№ҚдёҖзңӢж ҮйўҳвҖ”вҖ”гҖҠиӯҰжғ•пјҒпјҒдёӯиҚҜдјҡдҪҝйқ¶еҗ‘иҚҜзҡ„
 иӮҝзҳӨжӮЈиҖ…жғіеҗғдёӯиҚҜпјҢдёӯеҢ»жҸҗйҶ’дҪ дёҖе®ҡиҰҒ
дҪңиҖ…пјҡV
дёӯеҢ»жҳҜжІ»з–—иӮҝзҳӨзҡ„йҮҚиҰҒжүӢж®өд№ӢдёҖпјҢдҪҶдёҚз®ЎжҳҜеңЁз—…еҸӢзҫӨгҖҒи®әеқӣпјҢиҝҳжҳҜдёҙеәҠе®һи·өдёӯпјҢжҲ‘
иӮҝзҳӨжӮЈиҖ…жғіеҗғдёӯиҚҜпјҢдёӯеҢ»жҸҗйҶ’дҪ дёҖе®ҡиҰҒ
дҪңиҖ…пјҡV
дёӯеҢ»жҳҜжІ»з–—иӮҝзҳӨзҡ„йҮҚиҰҒжүӢж®өд№ӢдёҖпјҢдҪҶдёҚз®ЎжҳҜеңЁз—…еҸӢзҫӨгҖҒи®әеқӣпјҢиҝҳжҳҜдёҙеәҠе®һи·өдёӯпјҢжҲ‘
 еҮәеҖҚз‘һеҚҡ
еҘҪж—ҘжңҹпјҢеҲ°2025е№ҙпјҢ40дёҖ瓶гҖӮ
еҮәеҖҚз‘һеҚҡ
еҘҪж—ҘжңҹпјҢеҲ°2025е№ҙпјҢ40дёҖ瓶гҖӮ




 жҸҗеҚҮеҚЎ
жҸҗеҚҮеҚЎ зҪ®йЎ¶еҚЎ
зҪ®йЎ¶еҚЎ жІүй»ҳеҚЎ
жІүй»ҳеҚЎ е–§еҡЈеҚЎ
е–§еҡЈеҚЎ еҸҳиүІеҚЎ
еҸҳиүІеҚЎ еҚғж–ӨйЎ¶
еҚғж–ӨйЎ¶ жҳҫиә«еҚЎ
жҳҫиә«еҚЎ
